What is the 3-hour rule for diabetics? It's the idea that you should eat something roughly every three waking hours to keep blood glucose from swinging too far in either direction. The concept shows up in diabetes education materials, online forums, and well-meaning advice from friends, but it's an oversimplification of a much more nuanced topic.
Understanding what it actually means, and when it doesn't apply, can help you build a meal rhythm that genuinely works with your body, your medications, and your real life.
Here's the thing. There's no single official "3-hour rule" stamped by the American Diabetes Association (ADA). What does exist is the well-established principle that consistent meal timing supports steadier blood glucose, reduces hypoglycemia risk, and makes medication dosing more predictable.
How that principle translates into hours on a clock depends on your diabetes type, your drugs, your activity, and your own glucose patterns. Let's break it all down so you can figure out what actually fits your situation.
Quick Answer
The 3-hour rule for diabetics is a guideline suggesting you eat a meal or snack approximately every three waking hours. The goal is to prevent blood glucose from dropping too low or spiking too high between meals. It's not an official clinical standard.
The ADA recommends individualized meal planning instead of rigid intervals. People on insulin or sulfonylureas may benefit most from consistent timing. Those managing Type 2 with diet alone often have more flexibility.
What the 3-Hour Rule Actually Means
At its core, the 3-hour rule is about spacing your food intake so your blood glucose doesn't have time to crater or skyrocket between meals. The reasoning is straightforward. If you eat lunch at noon and don't touch food again until 7 p.m., that's a seven-hour gap.
For someone whose medication is actively lowering blood sugar during that window, those last two or three hours can get dangerous.
A 2023 review in Diabetes Care noted that irregular meal timing is associated with higher glucose variability, which itself is an independent risk factor for cardiovascular complications even when A1C looks acceptable. That's the real problem the rule tries to solve. Not just highs and lows you can feel, but the silent damage that glucose swings cause over months and years.
When people say "eat every three hours," they're really saying: don't leave long unbroken gaps where your medication is working without food coming in to match it. The three-hour window is a rough middle ground, short enough to prevent most hypoglycemia episodes but long enough to be realistic for daily life.
What the rule does NOT say is that you must set an alarm and eat identical portions regardless of hunger, activity, or what your glucose monitor is telling you. That rigid interpretation is where most of the problems start.
Why Meal Timing Matters for Blood Sugar Management
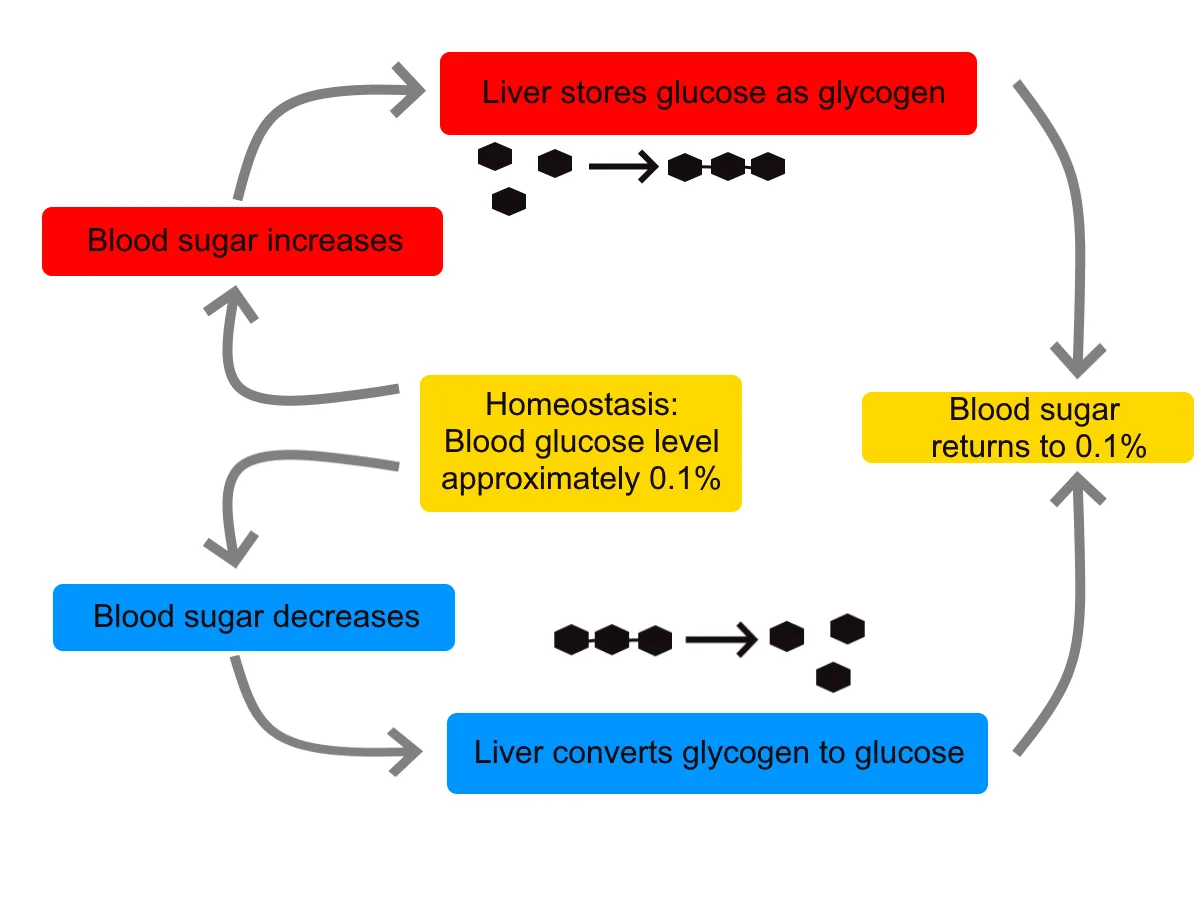
Blood glucose doesn't exist in a vacuum. It's the result of what you eat, what your liver is doing, what your medication is doing, and how active you are, all layered on top of each other throughout the day. Meal timing is one of the few variables you can control directly.
Here's why it matters in practical terms:
Insulin action windows are predictable. Rapid-acting insulins like lispro (Humalog), aspart (Novolog), and faster aspart (Fiasp) peak around 60 to 90 minutes after injection and remain active for roughly 3 to 5 hours. If you take a dose at mealtime but delay eating, you're asking for a low. If you eat a huge gap after the insulin has mostly worn off, your next meal may spike higher than expected.
Your liver keeps dumping glucose overnight. The dawn phenomenon raises fasting blood glucose in many people with diabetes, driven by growth hormone and cortisol surges between 4 a.m. and 8 a.m. Skipping breakfast after an overnight fast on top of that hormonal push can leave your body with neither food intake nor stable glucose for 12-plus hours.
Glucose variability drives complications. Research published in The BMJ (2019) found that high glycemic variability correlates with increased oxidative stress and endothelial dysfunction, even in patients whose average glucose (A1C) is at target. Spreading food more evenly across the day tends to flatten those peaks and valleys.
Appetite regulation improves. Going too long without eating often leads to extreme hunger, which leads to oversized portions, which leads to oversized spikes. It's a cycle that's hard to manage with medication alone.
How the 3-Hour Rule Works in Practice
Let's make this concrete. Say you wake up at 7 a.m., take your morning medication or insulin, and eat breakfast at 7:30. Three hours later, it's 10:30 a.m.
The rule suggests having a small snack or planning lunch right around that window. Lunch at noon or 12:30 keeps the rhythm going. Then another three hours puts you at 3:30 p.m., which might be a snack or an early dinner depending on your schedule.
Here's what that could look like in a typical day:
| Meal | Approximate Time | Purpose |
|---|---|---|
| Breakfast | 7:30 a.m. | Breaks overnight fast; matches morning insulin or meds |
| Mid-morning snack | 10:30 a.m. | Catches tail end of bolus insulin; prevents pre-lunch low |
| Lunch | 12:30 p.m. | Refuels before afternoon dip; keeps afternoon glucose stable |
| Afternoon snack | 3:30 p.m. | Bridges gap to dinner; prevents exercising on low blood sugar |
| Dinner | 6:30 p.m. | Last major meal; timing affects overnight glucose patterns |
This isn't a prescription. It's a template you adapt. The key variables are your medication schedule, your activity level, your actual blood glucose readings, and whether you're even hungry at those times.
For people on intensive insulin regimens, particularly those using multiple daily injections (MDI), this pattern often emerges naturally because bolus doses need to be matched to carbohydrate intake. For someone managing Type 2 with metformin alone and no hypoglycemia risk, the rule matters much less because their medication doesn't force glucose downward the way insulin does.
One practical approach is to check your blood glucose before each planned eating time. If you're at 110 mg/dL and stable at the 3-hour mark, a moderate snack makes sense. If you're at 180 mg/dL and still coming down from the last meal, that snack can probably wait.

When the 3-Hour Rule Makes Sense and When It Doesn't
Blanket meal timing advice fails because diabetes management is deeply individual. The rule fits some situations well and falls apart in others.
When it genuinely helps:
- You're on rapid-acting or short-acting insulin timed to meals. Consistent spacing reduces the risk of stacking doses or missing coverage windows.
- You take sulfonylureas (glipizide, glyburide, glimepiride). These drugs stimulate insulin release regardless of food intake, making them the oral medications most likely to cause hypoglycemia.
- You've had recent episodes of low blood sugar. A structured eating schedule is one of the simplest interventions to reduce recurrences.
- You're newly diagnosed and overwhelmed. Having a predictable meal rhythm is a starting framework while you learn to read your body's signals.
- You're managing gestational diabetes, where tighter glucose targets and more frequent monitoring make structured timing a standard part of most care plans.
When it needs significant modification:
- You're on a basal-only insulin regimen with no mealtime insulin. Your long-acting insulin covers background needs and doesn't require strict mealtime matching.
- You use an insulin pump or automated insulin delivery system. These devices adjust basal rates in real time, giving you more flexibility with when and how much you eat.
- You manage Type 2 with metformin, GLP-1 receptor agonists, DPP-4 inhibitors, or SGLT2 inhibitors alone. These medications carry minimal to no hypoglycemia risk when used without insulin or sulfonylureas.
- You're practicing time-restricted eating or intermittent fasting under medical supervision. This shifts the goal from spacing meals to optimizing within fewer, larger eating periods.
- You work irregular hours or shift work. A rigid 3-hour clock schedule may be completely incompatible with overnight shifts or rotating schedules.
The common thread is this: the tighter your blood sugar control needs to be and the higher your hypoglycemia risk from medication, the more meal timing matters. The lower your medication-related risk, the more you can let hunger cues and lifestyle drive your schedule.
How the Rule Changes Based on Your Diabetes Type and Medication
The single biggest reason the 3-hour rule gets misapplied is that people treat Type 1, Type 2, and gestational diabetes as if they work the same way physiologically. They don't, and the rule shifts accordingly.
Type 1 Diabetes
In Type 1, the pancreas produces little to zero insulin. Every unit of insulin is injected or pumped in, and carbohydrate intake must match that insulin. Postprandial blood glucose rises fastest in the 60 to 90 minutes after eating, which is exactly when rapid-acting insulin is also peaking.
If those two curves don't overlap well, you get either a spike (insulin too late) or a crash (food too late).
For someone on basal-bolus therapy, eating at predictable intervals makes the math work. Carbohydrate counting, insulin-to-carb ratios, and correction factors all depend on knowing when you're going to eat. A common approach is three meals with one to two snacks, each roughly 3 to 4 hours apart, with bolus doses timed 10 to 20 minutes before eating.
Type 1 management is also where CGM data becomes genuinely transformative. Trend arrows showing blood glucose dropping at 4 p.m. can prompt a snack before a low happens, even if the 3-hour schedule says it's not "time" to eat yet.
Type 2 Diabetes
Type 2 presents a much wider spectrum. Someone recently diagnosed and managing with diet and metformin has very different timing needs than someone who's been on insulin for 15 years.
For those managing with lifestyle changes or metformin alone, the primary goals are reducing overall carbohydrate load, improving insulin sensitivity, and avoiding large post-meal spikes. Meal timing is less critical because the medication isn't actively pushing glucose downward between meals. Many people in this category do well with three meals a day and no forced snacks.
For those on sulfonylureas, the rule tightens up. These medications stimulate pancreatic beta cells to release more insulin regardless of blood glucose levels. Since the drug action isn't glucose-dependent, a missed or delayed meal after taking a sulfonylurea can cause hypoglycemia.
For Type 2 patients on basal insulin, the situation resembles a hybrid. The basal insulin provides steady background coverage, so large gaps between meals are less dangerous than they'd be with mealtime insulin. Still, eating at roughly consistent times each day helps the basal dose work as intended.
For those on basal-bolus regimens, the timing considerations mirror those of Type 1. Carb counting, insulin-to-carb ratios, and consistent spacing all become important again.
Gestational Diabetes
Meal timing during pregnancy with gestational diabetes is typically more structured than in other diabetes types. The hormonal environment of pregnancy increases insulin resistance as gestation progresses, and post-meal glucose targets are stricter. Most obstetric guidelines recommend three meals and two to three snacks daily, spaced roughly 2.5 to 4 hours apart.
The stakes are also different. Hyperglycemia in gestational diabetes drives fetal macrosomia, neonatal hypoglycemia, and increased risk of cesarean delivery. So while the rule isn't called the "3-hour rule" in clinical practice, the practical effect is very similar.

Common Mistakes People Make With Meal Timing
The 3-hour rule sounds simple, but the most common errors come from applying it too rigidly without considering what's actually happening with your glucose levels and medication.
Snacking by the clock, not by need. Eating every three hours whether you're hungry or not adds calories and can drive weight gain and higher average glucose. If your pre-snack reading is 160 mg/dL, that snack is likely doing more harm than good.
Ignoring CGM or meter data. Your glucose monitor doesn't care what time it is. If your CGM shows 95 mg/dL with a steady arrow two hours after eating, waiting another hour for your scheduled snack is arbitrary. If you're dropping at 120 mg/dL with a down arrow at the two-hour mark, eating early is the right call.
Eating the same size snack every time. A three-hour gap after a light salad requires a very different snack than a gap after a pasta dinner. Portion and carbohydrate content should scale with what you ate and what your glucose is doing.
Forgetting about the dawn phenomenon. Eating breakfast at 8 a.m. after rising at 6 a.m. means your body has been fighting rising glucose for two hours with no incoming fuel. For many people, eating within an hour of waking makes a meaningful difference in daytime stability.
Not adjusting for exercise. Physical activity increases insulin sensitivity and can lower blood glucose for hours afterward. If you exercise at 5 p.m. and your usual snack time is 6:30 p.m., you may need that snack earlier or in larger quantity to prevent an evening low.
Stacking insulin doses. If the rule tells you to eat at 3 p.m. and you take rapid-acting insulin at 2:50 p.m., but then don't actually eat until 3:20 because something came up, you've created a mismatch. The insulin is peaking while your glucose is still processing lunch. This is one of the more dangerous timing errors.
How to Build a Meal Schedule That Actually Works for You
Forget the clock for a moment. Building a meal schedule that genuinely supports your blood sugar management is a four-step process grounded in your actual data, not a generic template.
Step 1: Establish your baseline pattern. For one full week, eat as you normally would and check your blood glucose before each meal, one hour after each meal, and at bedtime. If you use a CGM, even better. You're looking for patterns.
Do you consistently spike after breakfast? Drop at 4 p.m.? Wake up high?
Those patterns tell you where timing matters most for your body.
Step 2: Map your medication to your meals. Write down exactly what you take and when. Note the onset time, peak time, and duration. Your pharmacist or Certified Diabetes Care and Education Specialist (CDCES) can help with this if your prescription labels are unclear.
| Medication Type | Onset | Peak | Duration | Timing Implication |
|---|---|---|---|---|
| Rapid-acting insulin (lispro, aspart) | 10-20 min | 60-90 min | 3-5 hours | Must eat within 15-20 min of injection |
| Short-acting insulin (Regular) | 30 min | 2-3 hours | 5-8 hours | Eat within 30 min; longer gaps between meals help |
| Long-acting insulin (glargine, degludec) | 1-2 hours | Minimal peak | 12-42 hours | Background coverage; meal timing more flexible |
| Metformin | 1-2 hours | N/A | 12-24 hours | Low hypoglycemia risk; timing less critical |
| Sulfonylureas (glipizide) | 30 min | 1-3 hours | 12-24 hours | Must eat on schedule; hypoglycemia risk is real |
Step 3: Set your anchor times. Pick your breakfast time first. This is your anchor because it breaks the overnight fast, which for most people is the longest glucose-unstable window. Then work outward.
If you eat breakfast at 7:30 a.m. and your medication profile suggests 3- to 4-hour spacing, lunch lands around 11:30 a.m. to noon. Dinner follows 4 to 5 hours later.
Step 4: Adjust based on data, not dogma. After two weeks on your new schedule, review your glucose log. If your 3 p.m. reading is consistently below 80 mg/dL, your afternoon gap is too long or your lunch portion needs adjustment. If your pre-dinner reading is above 180 mg/dL despite correct timing, the issue may be your lunch composition rather than the clock.
The goal isn't a perfect 3-2-3-2 hour cadence. It's a rhythm that keeps your time in range (the percentage of readings between 70 and 180 mg/dL) as high as possible. Per ADA-aligned targets, most adults with diabetes should aim for above 70% time in range.
What the Research and Guidelines Say About Eating Intervals
The ADA's Standards of Care (updated annually, 2024 edition current as of this writing) don't prescribe a specific number of hours between meals. What they do state clearly is that meal planning should be individualized, and that consistency in carbohydrate intake at meals and snacks can improve glycemic outcomes. That's a meaningfully different framing than a rigid hour-based rule.
A 2019 meta-analysis published in Nutrients examined meal frequency studies in Type 2 diabetes. Higher meal frequency (5 to 6 smaller meals versus 3 larger ones) showed modest benefits for body weight and post-meal glucose, but the effect on A1C was inconsistent across studies. The takeaway: more frequent eating may help blunt spikes, but the total carbohydrate load matters more than the clock.
For patients using continuous glucose monitoring, the concept of "time in range" has shifted how clinicians think about meal timing. Rather than asking "did you eat on schedule?", a CDCES or endocrinologist reviewing CGM data is more likely to ask "where are your glucose curves going out of range, and what's happening at those times?". That's a data-first approach that often overrides generic rules.
The UK's National Health Service (NHS) diabetes dietary guidance echoes the individualized approach, recommending that people spread food intake across the day but stopping short of mandating specific intervals. Their practical guidance focuses on carbohydrate awareness, portion control, and choosing lower glycemic index foods, with timing as a secondary consideration.
Snacking, Hypoglycemia, and Staying Safe Between Meals
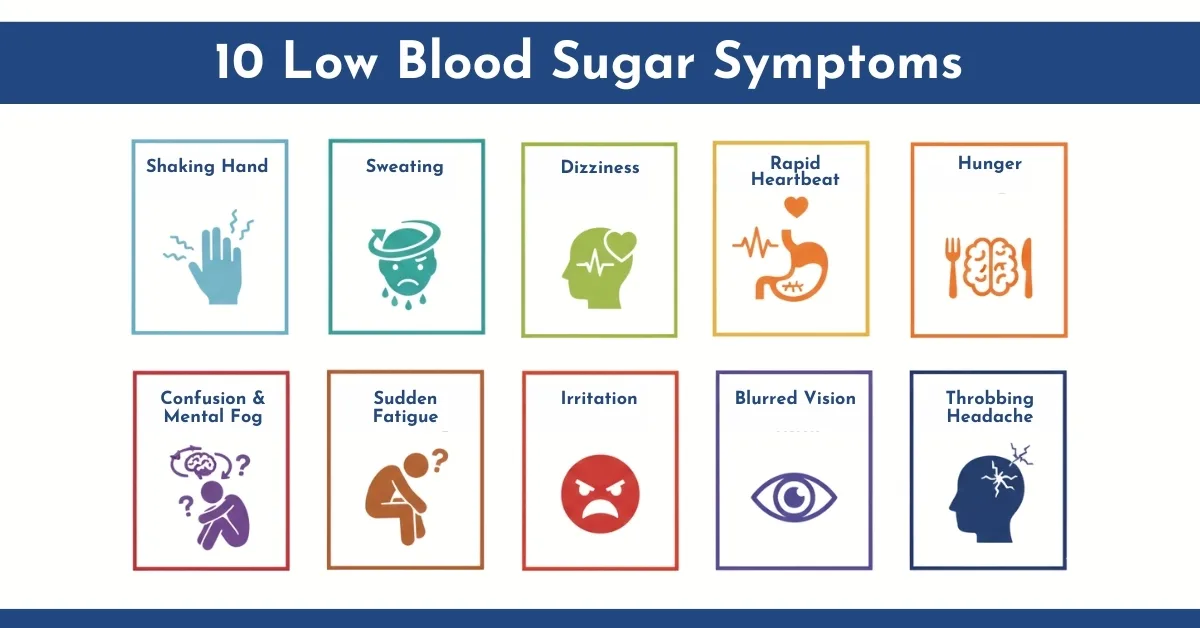
The whole reason the 3-hour rule exists is to prevent hypoglycemia, blood glucose dropping below 70 mg/dL. For people on insulin or sulfonylureas, a gap that's too long can turn dangerous fast. Symptoms start mild.
Shakiness, sweating, irritability, difficulty concentrating. Below 54 mg/dL, you're in clinically significant territory. Confusion, loss of coordination, and in severe cases, seizures or loss of consciousness.
The rule of 15 is the standard first-line response. Consume 15 grams of fast-acting carbohydrates, wait 15 minutes, recheck your blood glucose. If you're still below 70 mg/dL, repeat.
Glucose tablets, 4 ounces of juice, or a tablespoon of honey all deliver roughly 15 grams. Once you're back above 70 and stable, eat a small snack with protein and complex carbs to prevent a second drop.
Keep fast-acting carbs within arm's reach at all times. Nightstand, glove compartment, desk drawer, gym bag. If you're on a medication that can cause lows, treating them quickly isn't optional.
It's the difference between a minor inconvenience and a 911 call.
How CGM Data Can Help You Fine-Tune Your Timing
Continuous glucose monitors have fundamentally changed how people with diabetes approach meal timing. Instead of guessing whether a 3-hour gap is right for you, a CGM shows you exactly what your glucose is doing in real time. Devices like the Dexcom G7, Abbott Libre 3, and Medtronic Guardian 4 read interstitial glucose every one to five minutes and display the result on your phone or receiver.
The most useful feature for meal timing is the trend arrow. A single reading of 110 mg/dL means something different if the arrow is pointing straight down versus holding flat. A downward trend at 110 means you'll likely be at 80 within 20 minutes.
That's your signal to eat now, not in an hour when the schedule says it's time.
Over two to four weeks of CGM wear, patterns emerge. You might discover that your glucose consistently drops between 3 p.m. and 4 p.m. on days you eat a low-carb lunch. Or that your overnight readings stay flat when dinner finishes by 7 p.m. but climb when you eat at 9 p.m.
These patterns let you personalize your timing in ways a generic rule never could.
Time in range is the metric that ties it all together. If your TIR is above 70% and your hypoglycemia burden is below 4%, your current timing is working regardless of whether it follows a 3-hour cadence.

Frequently Asked Questions About the 3-Hour Rule
Do I have to eat every 3 hours if I have diabetes?
No. The 3-hour interval is a guideline, not a mandate. Your ideal spacing depends on your medication, your glucose patterns, and your daily routine.
Some people do well with 4-hour gaps. Others need something closer to 2.5 hours after certain meals. The goal is avoiding long stretches where your medication is active without food to match it.
What happens if I skip a meal and my timing is off?
If you're on insulin or a sulfonylurea and you skip or significantly delay a meal after taking your dose, your blood glucose can drop into hypoglycemic range. Symptoms include shakiness, sweating, confusion, and in severe cases, loss of consciousness. Always carry fast-acting carbohydrates.
If you know you'll miss a meal, talk to your care team about adjusting your dose in advance.
Is the 3-hour rule different for Type 1 and Type 2 diabetes?
Yes, significantly. In Type 1, every meal requires matching insulin to carbohydrate intake, so consistent timing directly affects dosing accuracy. In Type 2 managed with metformin or lifestyle alone, the rule matters much less because those treatments don't cause hypoglycemia.
Type 2 patients on insulin or sulfonylureas fall somewhere in between, with timing importance scaling alongside hypoglycemia risk.
Can I use intermittent fasting if I have diabetes?
Some people with Type 2 successfully use time-restricted eating under medical supervision. This compresses all daily calories into a 6- to 8-hour window, which is the opposite of the 3-hour spacing approach. It requires careful medication adjustment and close glucose monitoring.
It is not appropriate for anyone on insulin or sulfonylureas without direct oversight from their endocrinologist.
How do I know if my meal timing is working?
Check your time in range. If over 70% of your readings fall between 70 and 180 mg/dL, and you're spending less than 4% below 70, your timing is doing its job. Review your glucose data weekly.
Look for recurring patterns at specific times of day. Adjust your schedule based on what the data tells you, not on a generic rule.
The Bottom Line on Meal Timing for Diabetes
The 3-hour rule is a useful starting framework, not a clinical standard. It captures a real principle: consistent meal spacing helps stabilize blood glucose, especially for people on insulin or sulfonylureas. But the rigid version of the rule, eat every three hours no matter what, ignores the enormous variation in how diabetes works from person to person.
Your medication profile is the single biggest factor in how much timing matters. Rapid-acting insulin demands precision. Metformin does not.
Your CGM data is more valuable than any generic schedule. And your care team, your endocrinologist, your CDCES, your registered dietitian, can help you build a plan that accounts for your specific physiology, your medications, and your life.
Start with consistency. Eat at roughly the same times each day for two weeks. Track your glucose before and after meals.
Look for patterns. Then adjust based on what you see. That iterative process will get you further than any rule pulled from a headline.